Step 2
The Clinical Problem
A client arrives complaining of pain deep in the buttock that travels down the back of the leg.
They may report burning, tingling, or shooting pain that extends through the thigh and sometimes even into the calf or foot. Sitting for long periods often makes the pain worse, and standing or walking may feel unstable or uncomfortable.
This pattern of symptoms is commonly described as sciatica.
Many explanations for sciatica focus on the lower back, suggesting that a spinal disc or vertebra is compressing the nerve. While spinal causes do occur, a very common and often overlooked source lies in the piriformis muscle.
The piriformis runs from the sacrum to the femur and lies directly beside the sciatic nerve, the largest nerve in the body.
When the piriformis enters spasm, it can compress the sciatic nerve as the nerve passes through the deep gluteal region. Because the sciatic nerve carries signals to the entire back of the leg, even mild compression can produce intense radiating pain.
When the piriformis contracts strongly or remains in spasm, it can also tilt the sacrum. Because the sacrum forms the base of the spine, this tilt can alter the relationship between the sacrum and the fifth lumbar vertebra (L5).
This change in alignment may narrow the space where the lumbar nerves exit the spine, creating additional irritation of the nerves that contribute to the sciatic nerve.
Clients may therefore experience symptoms that seem to originate from both the hip and the lower back.
Common symptoms include:
• deep pain in the buttock
• radiating pain down the back of the leg
• burning or tingling sensations in the leg
• increased pain when sitting
When the piriformis muscle is released, pressure on the sciatic nerve is relieved and the sacrum can return to its natural position beneath the spine.
For this reason, releasing the piriformis often produces rapid relief of sciatic nerve symptoms and restores normal movement to the hip and lower back.

The piriformis muscle
To relieve sciatica, simply release the piriformis muscle.
 Deep Hip External Rotators |  Quadratus Femoris | 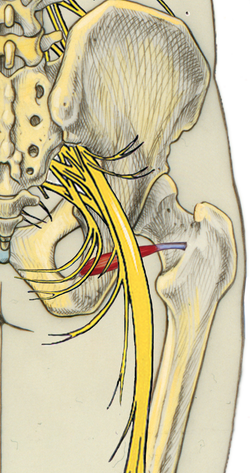 Gemellus Inferior |
|---|---|---|
 Obturator Externus | 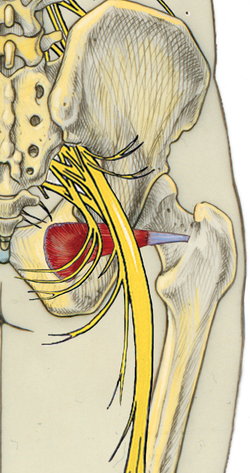 Obturator Internus |  Gemellus Superior |
Other nearby muscles — including the gemellus, obturator, and quadratus femoris — lie along the same pathway and can produce aching or soreness in the buttock when they become tight. However, these muscles rarely produce the true radiating nerve pain associated with sciatica.The piriformis is the muscle most capable of directly compressing the sciatic nerve.
Step 3
Why This Happens
The Root Cause of Muscle Spasm
Muscle spasm is not tightness.
It is not a flexibility problem.
A muscle spasm is an involuntary contraction caused by fatigue of the muscle cells.
When metabolic fatigue accumulates inside the muscle fibers, the cells lose their ability to release calcium and the muscle becomes locked in contraction.
What Happens Inside the Muscle
When enough fibers cross this metabolic threshold, the muscle loses its ability to relax and becomes locked in spasm.
This persistent contraction:
• reduces blood flow
• traps metabolic waste products
• increases neural irritation
The muscle becomes a localized metabolic crisis.
Why the Scalenus Creates Neurological Symptoms
The scalenus anterior sits at the entrance to the thoracic outlet.
When the muscle becomes locked in spasm, it narrows the space through which several neurological and vascular structures must pass.
Even small changes in this space can interfere with normal nerve and blood flow.
Why Symptoms Appear Far From the Neck
As the muscle contracts and shortens, blood flow is reduced and neural conductivity becomes impaired.
This is why symptoms can appear far from the neck itself.
Migraines, arm symptoms, breathing disturbances and nervous system irritation may all originate from this muscular bottleneck.
Releasology does not chase symptoms.
It releases the cause.

Scalenus anterior (red) running from the cervical vertebrae to the first rib. Spasm in this muscle narrows the thoracic outlet and compresses nearby neurological structures.
Step 4
Anatomy
The scalenus anterior originates from the transverse processes of the cervical vertebrae and inserts on the first rib.
Its position places it directly adjacent to several critical neurological and vascular structures.
Structures influenced by scalenus anterior spasm include:
• Brachial plexus
• Phrenic nerve
• Vagus nerve
• Carotid artery
• Cervical nerve roots
Because these structures pass directly beside the muscle, even a small contraction can produce significant neurological effects.

Step 5
Accessory Muscles
The scalenus anterior does not act alone.
It functions as part of a coordinated group of cervical stabilizers.
Primary muscle:
• scalenus anterior
Accessory muscles:
-
Scalenus anterior
-
Scalenus medius
-
Scalenus posterior
-
Sternocleidomastoid
-
Levator scapulae
-
Upper trapezius
These muscles often become painful and hypertrophic because they are compensating for instability created by anterior cervical collapse.






Step 6 — Neurological Consequences
When the scalenus anterior enters spasm, it can compress multiple neurological pathways.
Anterior cervical spasm traps:
-
Cervical nerve roots
-
Sympathetic fibers
-
Autonomic signaling pathways
This produces symptoms such as:
• Migraines
• Neck pain
• Radiating arm symptoms
• Nervous system irritation
• Breathing changes
• Nausea in severe cases
When cervical pain is accompanied by nausea, vagus nerve involvement should be suspected.
Understanding these neurological relationships allows the practitioner to identify the correct release protocol.
Step 7 — Technique Demonstration
Watch the following technique demonstration carefully.
Pay attention to:
• practitioner stance
• hand placement
• body mechanics
• direction of pressure
• the Yang–Yin release cycle
Releasology pressure is not force.
Pressure is information delivered through correct body mechanics.
The practitioner applies controlled Yang compression until the tissue reaches the release threshold.
Pressure then softens into the Yin phase, allowing the muscle fibers to relax.
Step 8 — Worksheet Exercise
Download the worksheet below.
Using a red drawing tool on your phone or tablet:
-
Trace the attachments of the scalenus anterior.
-
Identify the cervical vertebrae involved.
-
Mark the first rib insertion.
-
Review the surrounding neurological structures.
Save the image to your device.
Upload the completed worksheet in the next step.
Mastery of anatomy is required for precise clinical work.
Step 9
Practice Assignment
Clinical Skill Development
Set up a massage table and recruit a practice subject for your first scalenus anterior release.
If possible, choose a subject experiencing::
• neck pain
• migraines
• arm symptoms
• breathing restriction
Watch the technique video again and pause frequently.
Practice slowly until you can clearly feel:
• correct finger positioning
• correct practitioner body mechanics
• the Yang engagement phase
• the Yin release phase
The goal is not force.
The goal is precise engagement of the tightest fibers.
Once you have performed the release successfully, proceed to the next step.
Step 10
Technique Recording
In this step you will record yourself performing the scalenus anterior release technique so your form and body mechanics can be evaluated.
You will need:
• a massage table or treatment surface
• a practice subject
• a tripod or stable support for your phone or camera
• good lighting so your hand placement is clearly visible
Position the camera so that the following are clearly visible in the video:
• your hand placement on the client
• your body mechanics and posture
• the direction of pressure you apply
• the client’s neck and shoulder region during the release
The video should show the entire treatment sequence, from initial contact to release.
Record yourself performing the scalenus anterior release technique so your form and body mechanics can be evaluated.
☑ correct finger placement
☑ practitioner body mechanics
☑ the Yang engagement phase
☑ the Yin release phase
The video should show the full treatment sequence from initial contact to muscle release.
Upload your video for instructor review.
Your instructor will confirm that the technique is performed safely, accurately, and according to the Releasology method.
This step allows your instructor to confirm that the technique is being performed safely, accurately, and according to the Releasology method.
Step 11
Client Testimonial
Ask your practice subject to rate their symptoms before and after the treatment using a 0–10 scale.
Record a brief testimonial video including::
☑ symptom description
☑ before score
☑ after score
☑ changes they experienced
Upload the testimonial video.
Documenting real clinical outcomes is an essential part of Releasology training.
Step 12
Knowledge Check & Module Completion
Complete the following quiz to confirm your understanding of the Scalenus Anterior Release technique and the key concepts in this module.
Modality Quiz
Complete the following quiz to confirm your understanding of the Scalenus Anterior Release technique. A score of 80% or higher is required to pass this module.
Scalenus Anterior Release Specialist
Congratulations!
You have completed the Scalenus Anterior Release Module.
You should now understand:
• the physiological cause of scalenus spasm
• the neurological structures affected
• the correct Releasology release protocol
• the clinical symptoms this modality resolves
You may now proceed to the next module in the Releasology system.